

Dr Amiee Vyas presents a case study on treating ageing and pigmentation with topical skincare
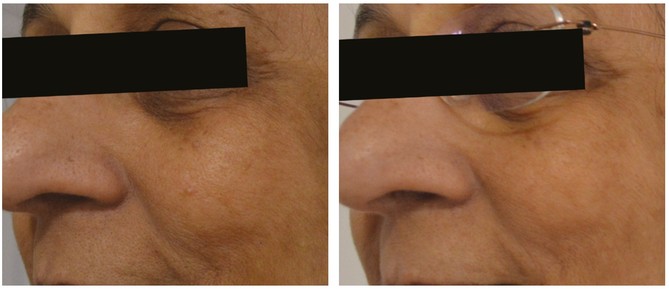
This is a case of a 73-year-old, Fitzpatrick skin type IV female of Indian origin who presented with visible signs of ageing. Her main concerns were uneven skin tone and hyperpigmentation, as well as an overall tired appearance. The hyperpigmentation was moderate in severity, consistent with her Fitzpatrick type and a significant history of unprotected sun exposure in her younger years. On examination with a Wood’s Light, the pigmentation was predominantly epidermal with some dermal patches. The patient had previous history of cosmeceutical use, but no history of aesthetic injectables or chemical peels and no past medical history or allergies to note. Her main aim was to improve her skin quality with non-invasive treatments, minimal downtime and no obvious skin shedding.
Treatment
The skin barrier is inevitably weakened with increased age due to intrinsic factors1 including slower cell turnover, reduced type I collagen production, hormonal changes, and reduced oil production by sebaceous glands, melanocyte changes and elastosis causing a disorganised connective tissue structure.2,3 This results in fine lines and wrinkles, dryness, skin laxity, uneven texture and tone, as well as enlarged, more visible pores, all of which are further exacerbated by extrinsic photodamage.2,3 I chose to address this patient’s concerns purely with topical skincare because her consultation revealed that she wanted a homecare regime without frequent clinic visits. She understood the benefit of combining homecare with in-clinic treatments such as chemical peels or medical microneedling, but she was not keen to proceed with these treatments because of the associated downtime. The patient was not worried about the speed of the result and was happy to see a gradual improvement over time. She understood that this could take three months or longer to visualise. She had realistic expectations and was aware that whilst we were working towards the best improvement for her skin, there would be no guarantee of resolution of her hyperpigmentation with homecare alone. The ‘gold standard’ topical treatment of skin ageing with retinol/retinoids (namely prescription strength tretinoin) and alpha hydroxy acids is well established in clinical practice through effects of exfoliation and promotion of skin turnover.4 Hence, these were the first ingredients I considered for my patient’s regime. Retinoids applied at night normalise skin structure by increasing cellular mitosis, thus stimulating collagen production, and can offer excellent benefits to pigmentation through tyrosinase inhibition and improved melanocyte function.2,5-8 However, compliance is often an issue due to irritation and shedding, particularly in darker Fitzpatrick skin types who can experience dermatitis in response to topical retinoids.9,10
I considered alpha hydroxy acids such as glycolic acid and lactic acid because of their ability to modulate both epidermal and dermal changes at high concentrations.11,12 This facilitates skin turnover and renewal of the stratum corneum, improving skin texture, fine lines, wrinkles and pigmentation,2,11 as well as directly accelerating collagen and elastin synthesis in the dermis.11,12,13
Extrinsic photoageing causes inflammation, which stimulates elastases to degrade elastin and causes dermal matrix degradation via disruption to the collagen fibre network.14 The production of reactive oxygen species secondary to UVA and UVB exposure exacerbate this degradation14 and also the visible signs of ageing. Glycolic acid has anti-inflammatory and antioxidant properties to mitigate these processes.3 Furthermore, it is safe to use in all Fitzpatrick skin types2,15,16 and, in my experience, is well tolerated if used in a stepwise, controlled manner. Lactic acid has well documented benefits of moisture retention to increase epidermal and dermal volume, thereby reducing fine lines and wrinkles and improving overall skin luminosity.2,17 By selecting products with these multimechanistic ingredients, I aimed to provide an effective regime for the patient that was simple to use without numerous steps.
With my patient being of South Asian descent, it was important to consider the differences in her ageing process compared to Caucasian and other skin types. Asian and Indian subjects are more susceptible to pigmentation disorders,18 which often manifest before visible rhytides in this patient group.19 To specifically target pigmentation and, in line with my patient’s requirement to avoid visible peeling, I sought to introduce a second non-retinoid, nonhydroquinone product to correct the skin tone.
Melanogenesis occurs in melanocyte organelles called melanosomes within the epidermis. It involves a cascade of events in which tyrosine is oxidised to dopa and then dopa is oxidised to melanin by the enzyme tyrosinase.7,20,23 This cascade, as well as the subsequent processes of melanin transport and distribution, all affect skin coloration.20 I aimed to target multiple pathways of melanogenesis and melanin distribution23 with novel ingredients to complement the effects of the topical retinoid and achieve the best outcome for my patient.
The most obvious difference between skin of colour and Caucasian skin types is the higher concentration of melanin in melanosomes.19 Furthermore, on a molecular level, specific pigmentation genes including some members of tyrosinase-related protein (TRP) family and melanocyte-stimulating hormone (MSH) also contribute to variations in pigmentation.19,24 Specifically, TRP-1 increases tyrosinase activity, melanin production and melanosome size.19,24 Arbutin is a naturally occurring derivative of hydroquinone without the melanotoxic effects; it inhibits both tyrosinase activity and melanosome maturation and its effects are dose dependant.27 The synthetic form alpha-arbutin has widely replaced the use of arbutin in topical products due to stronger tyrosinase inhibition and increased efficacy of depigmentation.27
Hexylresorcinol (HR), is another naturally-occurring agent affecting melanogenesis on multiple levels. It is an inhibitor of the tyrosinase,20,23 and peroxidase enzymes in the melanin cascade.20 HR has a stimulatory effect on glutathione,20 which is lost in the presence of UVA irradiation.28 Depletion of glutathione has been shown to increase tyroinsase activity29 and glutathione is also thought to have a dose dependant inhibition on melanin synthesis.20
Gallic acid is a naturally-occurring plant polyphenol antioxidant which has been shown in vitro to decrease melanin production by downregulating tyrosinase activity through down regulation of MITF and other melanogenesis-related proteins.26 It has also been found to be protective against UVB-induced hyperpigmentation.27
Finally, vitamin C was a key ingredient I looked for in product formulations because of its anti-pigmentary, antioxidative, photoprotective and overall antiageing effects30 through reducing matrix metalloproteinases production and collagen damage.30,31 It reduces pigment production by interacting with copper at tyrosinase active sites and inhibiting the action of tyrosinase.30,32-3
The oxidative effect of UV radiation has been suggested to contribute to melanogenesis,35,36 and vitamin C also neutralises oxidative stress by scavenging free radicals in a process of electron transfer.37 The Kakadu Plum has been shown to have the richest source of ascorbic acid and antioxidant potential.38,39 I therefore sought a formulation that could take advantage of this whilst remaining mindful that the benefits of topical vitamin C rest on its stabilisation from oxidation30 and hence looked for a product that utilised an appropriate delivery system.
The line I chose to use, which featured the ingredients I was looking for, was a skincare regime by skinbetter science. This included the AlphaRet Overnight Cream, Oxygen Infusion Wash and Even Tone Correcting Serum. I have found that fewer products are required in this home regime, which in turn helps to improve compliance, expedite results and enhance patient satisfaction. This was particularly important for my patient, who had previously used retinol and high strength alpha hydroxy acid-containing products, but found compliance difficult due to the number of steps in her regime. I instructed that the patient apply the Intensive AlphaRet formulation (containing a higher concentration of 18% glycolic acid for enhanced re-texturisation compared to the standard 10% formulation) at night. This was teamed with twice daily use of the Oxygen Infusion Wash and Even Tone Correcting Serum.
The patient also used a sunscreen with SPF 50 daily to prevent development of new pigmentation or exacerbation of existing areas via UV radiation mediated melanogenesis.18 She was advised to reapply this two hourly when exposed to the sun for long durations.
Despite her experience with active ingredients, I initially advised my patient to use the AlpharRet product alternate nightly for the first week and then increase to every night in order to increase tolerance and reduce irritation. The Even Tone Correcting Serum was used twice daily from the start, before the AlphaRet and before sunscreen.
Results
After nine months of using the skincare regime, a visible improvement was noted. The patient’s skin tone appeared brighter and more even, there was a significant reduction of pigmentation particularly noted on the cheeks and a global reduction of visible pores and wrinkles – particularly perioral lines, and softer nasolabial folds. The patient was extremely satisfied with the results, commenting, “I look younger than my youngest sister and I am six years older!” The patient reported that she tolerated the products with no irritation and found that the products could be used as advised from the outset without the need for more gradual use. This could be due to her previous experience of retinol and alpha hydroxy acid use, but could also be associated with the product’s technology, which allows for controlled gradual release of retinoid and lactic acid to minimise irritation potential.
Summary
Hyperpigmentation treatment is often challenging because of patient reluctance to accept the downtime associated with many procedures. Improvements can be made by topical skincare use and does not necessarily require irritating retinol and hydroquinone products or in-clinic procedures. Practitioners should choose a skincare line that includes active ingredients to best target their patient’s concerns and ensure maximum compliance. Patient selection is key and appropriate counselling regarding outcome is vital before commencing treatment plans based on homecare regimens alone.
